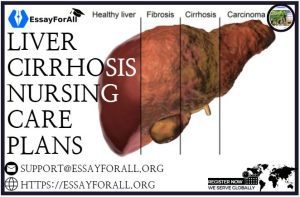
What is Liver Cirrhosis?
This condition involves the destruction and regeneration of liver cells leading to fibrosis throughout the liver. This can result in to change in liver structure, disrupt normal lymph and blood flow, and ultimately leads to hepatic insufficiency. This condition is caused by various factors like inflammation (caused by viruses or bacteria), malnutrition, and exposure to toxins such as carbon tetrachloride, alcohol, or acetaminophen. Liver cirrhosis is a significant threat to long-term health and a major cause of death among individuals aged 35 to 55 in the US.
Clinical types of Liver cirrhosis
- Pigment cirrhosis
- Postnecrotic Cirrhosis
- Noncirrhotic fibrosis
- Biliary Cirrhosis
- Laennec’s Cirrhosis
- Idiopathic Cirrhosis
Nursing Care Plans
The nursing care plans for liver cirrhosis patients involve providing enough nutrition, promoting rest, and skin care, minimizing risk for injury, and tracking and managing complexities.
Nursing care plans and nursing diagnoses for Liver Cirrhosis
- Deficient Knowledge
- Disturbed Body Image
- Excess Fluid Volume
- Imbalanced Nutrition: Less Than Body Requirements
- Risk for Ineffective Breathing Pattern
1.Deficient Knowledge
Cirrhosis can have a critical impact on individuals, families, and society as a whole. To effectively manage the disease and reduce its complications, educating the patient about Cirrhosis is significant so they can continue enjoying their lives. It is challenging to manage Cirrhosis; however, patients with the necessary knowledge can manage their health and enhance the long-term outcome. Health literacy pertains to an individual’s capacity to access, analyze, and understand crucial health information, enabling them to make appropriate decisions concerning their health.
Nursing Diagnosis
- Deficient Knowledge
It may be associated to
- Limited familiarity with sources of information
- Inadequate recall/exposure; misunderstanding of information.
Possibly evidenced by
- Inquiries; statement of misconception
- Not properly executing instructions and failing to
Nursing Assessment and Rationale
| Nursing Assessment | Rationale |
| Track disease prognosis, process, and future expectations. | This assessment is vital in creating a knowledge base that enables the patient to make informed decisions. |
| Identify potential environmental hazards like exposure to hepatitis. | Hepatitis C is the leading cause of Cirrhosis and chronic hepatitis in the US, although alcoholic liver disease was once the predominant cause of Cirrhosis. |
| Evaluate the degree of the client’s anxiety | The healthcare provider sees the client’s first stress upon receiving the diagnosis as the appropriate time to encourage changes in behavior and stimulate their motivation. |
| Evaluate the patient’s knowledge and awareness about their condition and treatment procedures. | Knowledge and awareness about the disease are essential in determining how the patient experiences the treatment procedures. |
| Evaluate the progression of the condition and forecast its outcome and future anticipation. | This is essential in providing a knowledge base for the patient to make informed decisions regarding their health situation. |
| Evaluate measures for maintaining peritoneovenous shunt functioning. | To ensure the Denver shunt is functioning correctly, the client must pump the chamber regularly; patients with a LeVeen shunt are recommended to wear an unusual binder or perform a Valsalva movement to keep the shunt functioning. |
Nursing Interventions and Rationale
| Nursing Interventions | Rationale |
| Refer the patient to a nutritionist or dietitian | Cirrhosis patients need close monitoring and appropriate nutritional advice. |
| Emphasis on avoidance of alcohol. | Alcohol is the primary cause of Cirrhosis |
| Educate the patient about the side effects of drugs on cirrhosis individuals. Emphasize the importance of prescribed medication or healthcare providers with clear client history. | Some medications are hepatotoxic (sedatives, hypnotics, and narcotics). Furthermore, the injured liver cannot metabolize some medication leading to increased bleeding. |
| Help the client to choose a support person. | The support system for cirrhosis patients is crucial in upholding lifestyle modification due to lengthy recovery, low healing, and potential for relapses. |
| Stress on good nutrition. Limit high-protein foods, strong cheese, and onions. To reinforce proper dietary intake, provide the patient with written instructions. | This is essential in averting ammonia buildup and liver damage. Written instructions provide the patient with a reference point at home. |
| Emphasis on follow-up care and compliance with the treatment program. | The chronic nature of Cirrhosis poses a possibly life-threatening complication. Thus, follow-up care helps assess the effectiveness of the treatment program. |
| Discuss with the patient about restrictions on sodium and substitute and the significance of reading food labels and OTC medications. | This is vital in reducing edema and ascites formation. Substitute usage may cause electrolyte imbalances. OTC, food, and personal care products like mouthwash and antacids may have alcohol or sodium. |
| Emphasis on scheduling tasks with enough resting periods. | Enough rest reduces metabolic needs in the body and preserves available energy for tissue regeneration. |
| Emphasis on diversional activities enjoyable to the client. | These activities help avert boredom and reduce depression and anxiety. |
| Stress on avoidance of people who may have infections, particularly URI. | Immuno-compromised patients are at high risk of infection. |
| Identify ecological hazards; exposure to hepatitis | Can increase the likelihood of recurrence |
| Educate the patient and SO on signs that need to be notified to healthcare providers, like fever, blood in urine or stool, rapid weight gain/loss, abdominal girth, and jaundice. | Timely reporting of signs lowers the likelihood of further hepatic damage and reduces complications. |
| Advise the SO to report any sign of confusion, night wandering, personality change, tremors, or untidiness. | So maybe more observant of the patient of changes indicating a decline, while individuals with less frequent patient interactions detect insidious changes that develop slowly over time. |
2.Disturbed Body Image
Cirrhosis affects the quality of life of the patient. The disease’s severity is linked to a compromised patient’s health-related quality of life (HRQOL). For instance, ascites cause breathlessness, abdominal discomfort, and increased anxiety and stress associated with physical appearance.
Nursing Diagnosis
- Disturbed Body Image
- Situational Low Self-Esteem
It may be associated to
- Personal vulnerability
- Self-destructive actions (alcohol-induced disease)
- Altered role function, the uncertainty of prognosis
- Altered physical appearance/Biophysical changes
Possibly evidenced by
- Feeling hopelessness, helplessness, or powerlessness
- A negative attitude about abilities/body
- Fear of rejection by friends and family
- Communication of restriction in lifestyle.
Possible nursing care outcome
- The patient is expected to identify feelings and coping techniques with negative self-perception.
- The patient is expected to demonstrate comprehension of the changes and accept themselves in the current condition.
Nursing Assessment and Rationale
| Nursing Assessment | Rationale |
| Evaluate the patient and family’s past coping techniques. | This helps in emphasizing those coping techniques that are effective and familiar to the patient. |
| Evaluate changes in appearance and what they mean to the patient and SO. | This helps provide information essential for evaluating the effects of changes in family roles, sexual function, and appearance on the patient and family. |
| Discuss the situation with the client and promote communication of concerns and fears. Explain how symptoms are related to the nature of the illness. | Clients are sensitive to self-alterations and may feel guilt when the condition is associated with drug or alcohol use. The treatment produces ascites, including nutritional restrictions, which impact HRQOL. |
Nursing Interventions and Rationale
| Nursing Interventions | Rationale |
| Encourage and support clients; provide care with a friendly and positive attitude. | Sometimes the caregivers may let their judgmental feelings impact their care of patients; thus, they need to exert themselves in ensuring that patient feels valued as individuals. |
| Encourage SO/patient communication of feelings, freely visit and participate in providing care. | The SO may be guilty because of the patient’s condition and feel fearful of anticipated death. Therefore, nonjudgmental support is recommended, and free access to the client. SO participation in patient care helps promote trust between them and healthcare providers. |
| Help the SO and the client to adapt to the altered appearance; encourage wearing clothes that do not show changes in appearance. | Due to jaundice, ecchymosis areas, and ascites, the client may present an unpleasant appearance; hence, emotional support is critical in enhancing their self-esteem and promoting a feeling of being in charge. |
| Refer the patient to the recommended support groups like psychiatric, counselors, clergy, social services, and alcohol treatment program. | The concerns and vulnerability related to this condition require additional professional support. |
3.Excess Fluid Volume
Ascites is a medical condition characterized by the buildup of excessive fluid within the abdominal cavity, and it can be a complication of non-liver-related or liver disease. People with liver cirrhosis may experience an accumulation of water and sodium and a decrease in the excretion of excess water, resulting in fluid overload in the body.
Nursing Diagnosis
- Excess Fluid Volume
It may be associated to
- Impaired minimized plasma proteins and regulatory mechanisms.
- Surplus fluid/sodium consumption
Possibly evidenced by
- Weight gain, anasarca, edema
- Adjusted CVP, BP changes
- Changed electrolyte volume
- Altered mental status.
- Adventitious respiratory sound, Dyspnea, pleural effusion
- Oliguria, higher intake than output, altered urine specific gravity
- Positive hepatojugular reflex, JVD
Possible nursing care outcome
- The patient is expected to demonstrate a stable fluid volume, weight, balanced consumption and output, and vital signs within the client’s optimal range, without edema.
Nursing Assessment and Rationale
| Nursing Assessment | Rationale |
| Evaluate breathing status and record breath rate and Dyspnea. | These signs signify pulmonary congestion. Portopulmonary hypertension, hepatopulmonary syndrome, hepatic hydrothorax, ventilation-perfusion mismatch, reduced oxygen saturation, hyperventilation, decreased pulmonary diffusion capacity, and hyperventilation is manifestations of Cirrhosis. |
| Listen to the lungs, like reducing breath sounds and adventitious sounds. | Various issues like consolidation, compromised gas exchange, and possible complications may cause a rise in pulmonary congestion |
| Track BP. Record JVD and distention of abdominal vein | An increase in BP is typically linked to excess fluid volume in the body; however, it is not always caused by fluid leaving blood vessels. Swelling in the external jugular and abdominal veins are linked with blood vessel congestion. |
| Track for cardiac dysrhythmias. Listen to heart sounds and note S3/S4 gallop rhythm development. | It may result from HF, electrolyte imbalance, and reduced coronary arterial perfusion. |
| Evaluate the extent of peripheral edema. | Water and sodium retention reduced albumin, and maximized antidiuretic hormone can result in fluids moving into the tissue. |
| Measure abdominal girth. | Helps in reflecting ascites resulting from lost plasma proteins. High fluid accumulation lowers circulation volume and creates a deficit (dehydration) |
| Track serial chest x-rays | Pulmonary edema, pleural effusions, and vascular congestion occur regularly. |
| Track electrolytes and serum albumin, especially sodium, and potassium. | Reduced serum albumin impacts the plasma colloid’s osmotic pressure, forming edema. |
Nursing Interventions and Rationale
| Nursing Interventions | Rationale |
| Measure input and output, weigh and record weight gain of 0.5 kg/day and higher. | This helps evaluate the circulation volume status, resolution, or developing fluid shifts and respond to the treatment program. Weight gain or positive balance signifies fluid retention. |
| Emphasis on bedrest in the presence of ascites. | It may promote urination while lying down. |
| Provide regular mouth care, such as random ice chips. | Reduces thirst sensation. |
| Restrict fluid and sodium as recommended. | Sodium restriction is essential in lowering fluid retention in extravascular spaces. Fluid restriction helps in correcting dilutional hyponatremia. |
| Provided the recommended medication | · Diuretics
· Potassium |
| Emphasis on the drug that should not be used or used with caution | Patients with ascites should avoid some drugs or use them cautiously, such as NSAIDs, because of the likelihood of developing hyponatremia, sodium retention, and kidney failure. |
| Prepare the patient for the recommended TIPS. | In ascites management, TIPS plays a significant role in reducing sinusoidal pressure. |
| Help the patient with peritoneovenous shunt insertion. | Denver and LeVeen shunts are devices used to allow ascites and proteins to return into the intravascular space. They help in reversing protein loss and relieving ascites in some patients. |
4.Imbalanced Nutrition: Less Than Body Requirements
Timely recognition and management of malnutrition are essential in managing patients with liver conditions from the compensated stage of Cirrhosis to liver failure. With increased diabetes and obesity linked to non-alcoholic fatty liver disease (NAFLD), nutritional imbalances are growing in patients with Cirrhosis.
Nursing Diagnosis
- Imbalanced Nutrition: Less Than Body Requirements
It may be associated to
- Abnormal bowel function
- Vomiting/nausea, anorexia, early satiety (ascites), indigestion
- Insufficient diet; inability to digest/process nutrients
Possibly evidenced by
- Imbalances in nutritional research
- Weight loss
- Altered bowel function and sounds
- Wasting/poor muscle tone
Possible nursing care outcome
- The patient is expected to experience limited signs of malnutrition
- The patient is expected to gradually increase weight towards the desired target while ensuring that the client’s laboratory values are adjusted appropriately for their needs.
Nursing Assessment and Rationale
| Nursing Assessment | Rationale |
| Assess the patient for malnutrition | Patient with Cirrhosis often experiences malnutrition due to low dietary intake caused by a preference for alcohol or poor food choices, leading to malabsorption syndrome. |
| Evaluate eating interests and ability to swallow, taste and chew. | These are the primary factors that impact the digestion and ingestion of nutrients. |
| Use nutritional screening tools to evaluate the nutritional status of the patient. | Patients with Cirrhosis should be evaluated for malnutrition and screened. |
| Evaluate the functional status of the patient. | The patient’s functional status can be evaluated immediately as they arrive for consultation. |
| Assess dietary intake via calorie count. | This is essential in providing necessary information about needs, intake, and deficiencies. |
| Weigh as recommended and compare changes in recent weight history, fluid status, and skinfold assessment. | Skinfold measurements help in evaluating changes in subcutaneous fat reserve and muscle mass. |
| Evaluate cirrhosis severity | The CTP system has been used for several years as the standard prognostic tool in patients with Cirrhosis. The CTP score predicts life expectancy in patients with acute Cirrhosis. |
| Evaluate the glycemic control of the patient | It is essential to evaluate patients’ glycemic control, especially in diabetic patients, and subsequent anti-diabetic drugs. |
Nursing Interventions and Rationale
| Nursing Interventions | Rationale |
| Emphasis on eating all foods, including supplementary diets. | The patient may select food and eat a few bites due to loss of appetite or malaise, nausea, and generalized weakness. |
| Instruct the patient to eat and provide justification for specific dietary recommendations. Assist the patient with feeding if they experience fatigue or have a caregiver to help feed them. Include the patient in meal planning to include their preferences in food choices. | The recovery process requires proper nutrition and diet. The patient may eat well when the preferred food is considered, and family is involved. |
| Provide small regular meals. | If the patient cannot handle big meals, it might be due to pressure in the abdomen or the presence of ascites. Eating small meals throughout the day and snacks at night is recommended to deal with energy malnutrition. |
| Encourage salt substitutes if recommended, and avoid ammonium. | Salt substitutes improve food flavor and help increase appetite, while ammonia increases the risk of encephalopathy. |
| Restrict alcohol intake, uncooked food, and high-fat foods. | Alcohol is unsafe for cirrhosis patients due to its possible cause of further dama to the liver and liver failure. |
| Emphasis on regular mouthwash before meals. | The patient is at risk of bleeding, sore gums, and bad taste resulting in anorexia. |
| Encourage uninterrupted rest periods before meals. | Conserving energy is essential in reducing liver metabolic requirements and helps cellular regeneration. |
| Uphold NPO status when recommended. | GI rest is essential in reducing liver demands, urea, and ammonia production in the GI tract. |
| Encourage tube feedings, lipids, and TPN if recommended. | This is significant in providing nutrients or supplementing diet in nauseated patients, anorexia to eat, and when esophageal varices obstruct oral intake. |
| Optimize the recommended intake of proteins | It is critical to optimize protein intake since there is an increase in overall body protein breakdown and a reduction in muscle protein synthesis. |
| Encourage recommended nutritional oral supplements. | Sufficient protein and calorie intake could be challenging, especially for patients with sarcopenia, and nutritional supplements are necessary. |
5.Risk for Ineffective Breathing Pattern
Pulmonary complications are common in both patients with or without liver conditions. There should be a distinction between these particular disorders from a significant lung disease like COPD, common in patients with liver illness but not pathogenically linked to liver cirrhosis.
Nursing Diagnosis
- Risk for Ineffective Breathing Pattern
Risk factors include
- Reduced energy, fatigue
- Reduced lung expansion, excess secretions
- Ascites
Possible nursing care outcome
- The patient is expected to uphold a regular breathing rhythm, free from cyanosis and Dyspnea, with an accepted range of ABGs and vital capacity.
Possibly evidenced by
- It is inapplicable. Signs and symptoms cannot be used to diagnose a potential risk. The nursing interventions for fluid volume deficit are focused on preventing the problem from occurring rather than treating it after occurring.
Nursing Assessment and Rationale
| Nursing Assessment | Rationale |
| Listen to breath sounds recording rhonchi, crackles, and wheezes. | This helps indicate impending complications. The adventitious respiratory sounds show the accumulation of secretions or fluids. |
| Track breathing depth, effort, and rate. | Dyspnea or rapid shallow breath may appear due to fluid accumulation or abdominal hypoxia. |
| Track serial ABGs, chest x-rays, vital capacity measurements, and pulse oximetry. | This helps reveal changes in breathing status, thus, leading to pulmonary complications. |
| Observe temperature. Record the presence of chills, color changes, increased coughing, and the character of sputum. | This helps in indicating the onset of infections, particularly pneumonia. |
| Track laboratory outcomes from renal function. | Hepatorenal syndrome is identified by a low creatinine clearance rate below 40 ml/minute or observing serum creatinine level above 1.5 mg/dl, low urine volume below 500 ml/day, and low urine sodium level below 10 mEq/L. |
| Assess changes in consciousness level. | Changes in mentation indicate breathing failure and hypoxemia, mostly accompanying hepatic coma. |
Nursing Interventions and Rationale
| Nursing Interventions | Rationale |
| Raise the head of the bed. | This enhances patient breathing by lowering pressure exerted on the diaphragm and reducing secretions of aspirinogen. |
| Encourage oxygen supplement as recommended. | This averts or treats hypoxia, and mechanical ventilation may be necessary in cases of inadequate oxygenation or respiration. |
| Prepare the patient for contrast-enhanced echocardiography. | The most effective technique for identifying enlargement of the blood vessels in the lungs is contrast-enhanced echocardiography with agitated saline. |
| Assist or prepare for acute care measures. | · Paracentesis
· Peritoneovenous shunt · Liver transplantation · TIPS |
| Educate the patient on the importance of garlic in the diet. | Garlic contains allicin significant in enhancing gas exchange. |